Aneurysms and subarachnoid hemorrhage
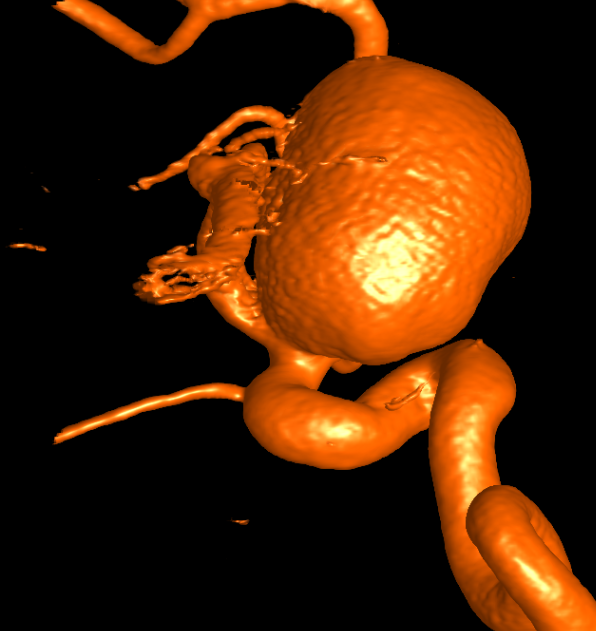
An intracranial aneurysm is a pathological vascular outpouching that is located on a vessel supplying the brain. Due to its thin walls, there is a risk that an aneurysm will rupture and cause cerebral haemorrhage (typically subarachnoid haemorrhage). The severity of the haemorrhage can vary from very mild to very severe and life-threatening.
An aneurysm that has bled once has to be treated, since the bleeding rate in the first days, weeks and months following the first haemorrhage is about 30-50%. Aneurysm treatment can also be carried out prophylactically for aneurysms that have not haemorrhaged and are discovered by chance (so-called "incidental" aneurysms). The risk of surgery or intervention must be weighed against the risk of haemorrhaging. The size and location of the aneurysm, certain risk factors and the patient's personal preference play a role here.
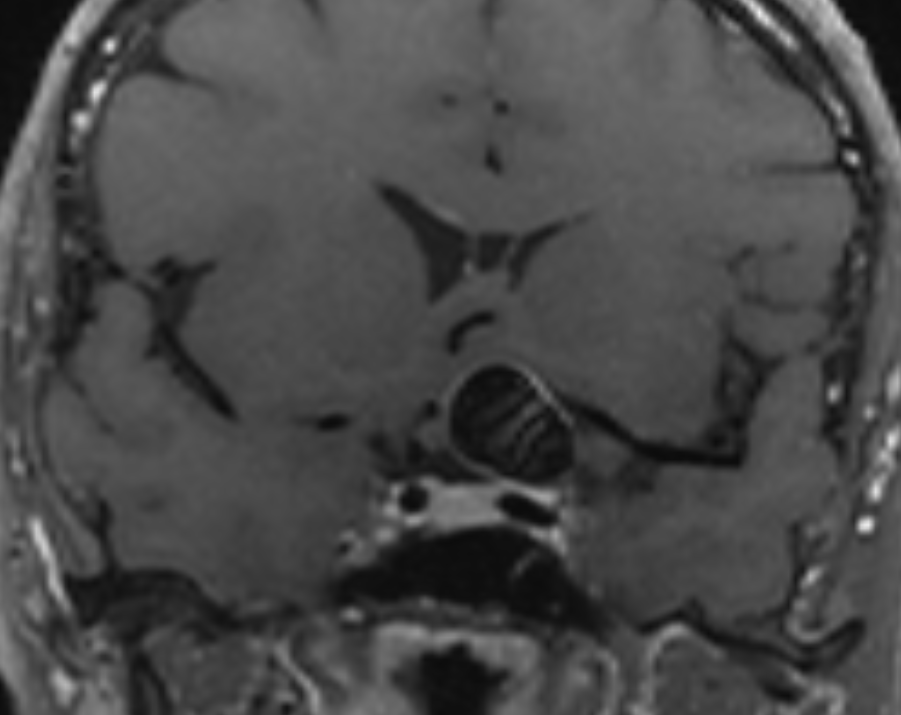
In principle, there are two treatment methods, neurosurgical (clipping) and neuroradiological (coiling), both aiming to prevent inflow of blood into the aneurysm and thus preventing (re)rupture. Aneurysm coiling is performed in an angiography suite. Under X-ray guidance using a contrast medium a microcatheter is navigated into the aneurysm and metal spirals (coils) are pushed through the microcatheter until the aneurysm is completely filled. Aneurysm clipping is a microsurgical procedure and is performed in the OR. The goal of the surgery is to close the neck of the aneurysm sac and reconstruct the lumen of the aneurysm-bearing artery with metal clips (titanium).
Brain MRI is an excellent non-invasive modality in the diagnostic work-up of brain aneurysms. Our research group focuses on imaging markers and risk factors in aneurysms to estimate rupture risks and guide treatment decisions. Furthermore, control algorithms after treatment and as well as in unruptured aneurysms are being investigated to determine sense full follow-up patterns for typical scenarios.